Aruna Shanbaug Euthanasia Case India: The Debate That Changed How We Think About the Right to Die
On the night of 27 November 1973, a young nurse at KEM Hospital in Mumbai was sexually assaulted and strangled with a dog chain by a ward boy. The attack cut off oxygen to her brain. She survived — but not in any way the word "survival" usually implies. For the next 42 years, Aruna Shanbaug lay in a persistent vegetative state, her body alive but her consciousness irretrievably lost.
Her case became India's most consequential legal battle over a question that medicine, law, religion, and philosophy have wrestled with for centuries: When life has no quality, does a person have the right to die? The Aruna Shanbaug euthanasia case India forced the Supreme Court to confront this question head-on — and the answers it gave reshaped Indian law permanently. If you want to understand euthanasia in India, where the law stands today, and why this debate is far from over, this is the article you need.
Who Was Aruna Shanbaug? The Story Behind the Landmark Case
Aruna Ramchandra Shanbaug was born in 1948 in Haldipur, Karnataka. She trained as a nurse and joined King Edward Memorial (KEM) Hospital in Mumbai, where she was working when her life was destroyed on a single November night.
The attack was carried out by Sohanlal Bhartha Walmiki, a hospital sweeper who assaulted Aruna in the hospital basement. He strangled her with a dog chain to immobilise her, cutting off blood and oxygen to her brain during the assault. The resulting brain damage left Aruna cortically blind, with severely compromised motor and sensory function. She was diagnosed as being in a persistent vegetative state (PVS) — a condition where the brain stem continues to function (enabling breathing and heartbeat) but higher brain functions are permanently non-functional.
What followed was extraordinary: the nurses and staff of KEM Hospital chose to care for Aruna for over four decades. She was fed through a tube, bathed, given medical attention, and kept alive in a hospital bed. Her case remained largely outside public consciousness until 2009, when journalist and activist Pinki Virani — who had written a book about Aruna — filed a petition before the Supreme Court of India seeking permission to withdraw the feeding tube sustaining her life.
Aruna Shanbaug passed away on 18 May 2015, not through any legal intervention, but from pneumonia — 42 years after the attack that took everything from her. Her case lives on as the defining moment in India's euthanasia jurisprudence.
What Is Euthanasia? Definitions, Types, and Key Terminology
Euthanasia is defined as the deliberate ending of a person's life to relieve them of prolonged suffering, typically due to a terminal or irreversible medical condition. The word derives from the Greek eu (good) and thanatos (death) — literally, a "good death." It is significant because it sits at the intersection of medical ethics, personal autonomy, and state authority over human life.
Types of Euthanasia
Understanding euthanasia requires distinguishing its several forms:
1. Voluntary Euthanasia: The patient consciously and explicitly requests death. This requires informed, competent consent.
2. Non-Voluntary Euthanasia: The patient is unable to give consent (e.g., in a coma or PVS), and the decision is made by a third party — family, court, or guardian.
3. Involuntary Euthanasia: Death is caused against the patient's expressed wishes. This is universally illegal and classified as murder.
4. Active Euthanasia: A deliberate act — administering a lethal injection or medication — directly causes death.
5. Passive Euthanasia: Life-sustaining treatment is withheld or withdrawn — such as removing a ventilator or feeding tube — allowing natural death to occur.
6. Physician-Assisted Suicide (PAS): The physician provides the means (medication, information) but the patient administers it themselves. Distinct from euthanasia where the physician acts directly.
- Euthanasia is not the same as palliative care or natural death
- The distinction between active and passive forms is legally critical in India
- Non-voluntary euthanasia applies directly to the Aruna Shanbaug situation
- Consent — or its absence — determines legality in most jurisdictions
- "Mercy killing" is a colloquial but legally imprecise synonym
The Aruna Shanbaug Case: Legal Journey from 1973 to 2015
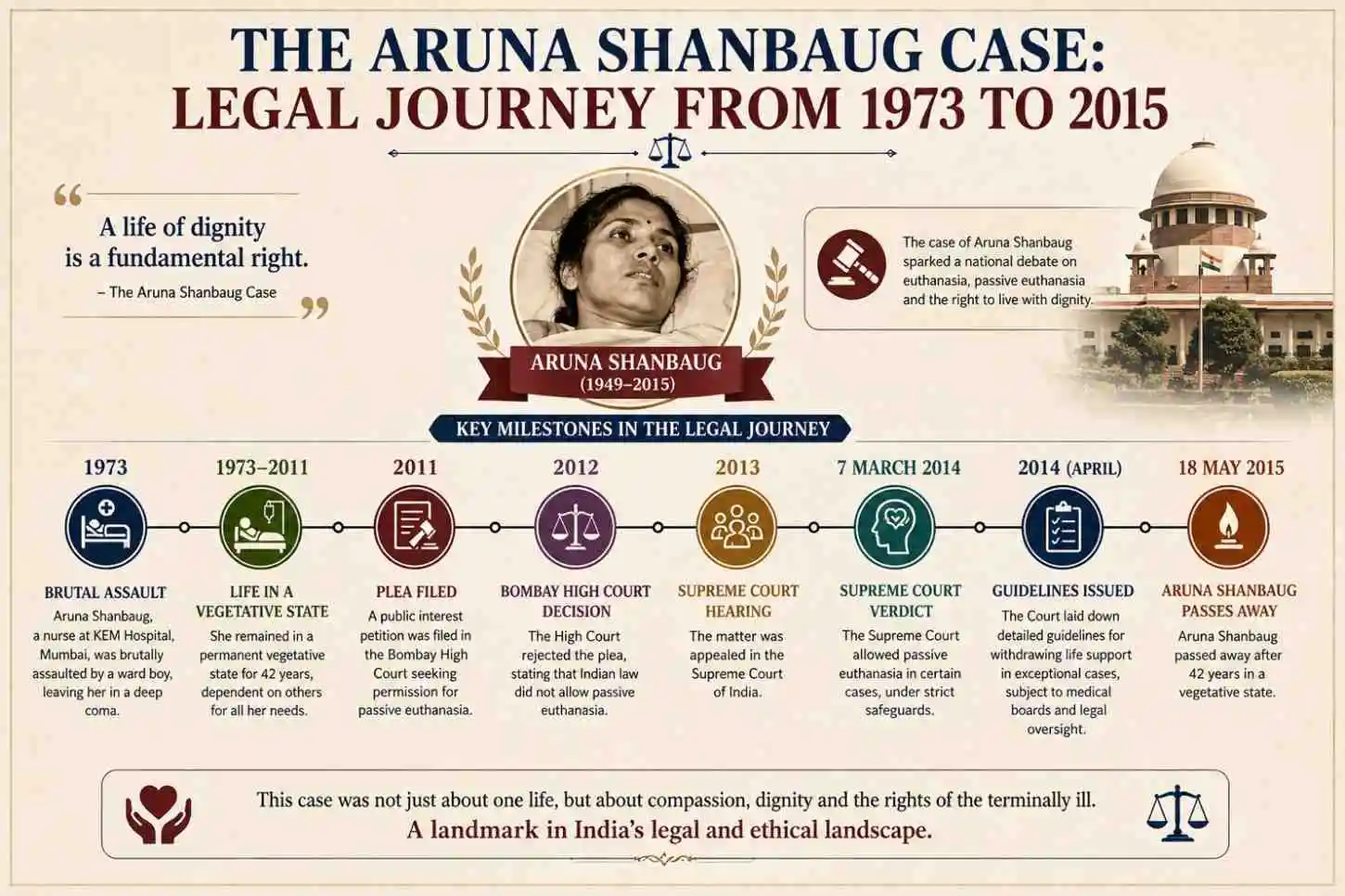
The legal story of the Aruna Shanbaug case is as layered as the ethical questions it raises. The criminal case against Sohanlal Walmiki resulted in his conviction — but only for robbery and attempted murder, not rape, because the medical examination had not established rape conclusively. He served a seven-year prison sentence and walked free. Aruna's suffering, meanwhile, lasted 42 years.
The euthanasia petition came four decades later. In 2009, Pinki Virani filed a writ petition under Article 32 of the Constitution before the Supreme Court, arguing that Aruna had the right to die with dignity under Article 21 (Right to Life and Personal Liberty). The petition specifically sought withdrawal of the feeding tube.
KEM Hospital opposed the petition. The nursing staff — who had cared for Aruna as their own — argued she responded to music, touch, and her environment, and that they did not want her to die. The hospital submitted that removing the feeding tube was not in Aruna's best interest.
The Supreme Court appointed a medical panel to examine Aruna and assess her condition. The panel confirmed she was in a persistent vegetative state with no possibility of recovery.
The 2011 Judgment: Aruna Shanbaug vs Union of India
On 7 March 2011, a two-judge bench of the Supreme Court delivered its landmark judgment in Aruna Ramchandra Shanbaug vs Union of India & Ors [(2011) 4 SCC 454]. The key findings were:
- Passive euthanasia was made conditionally legal in India — a historic first
- Active euthanasia remained illegal under Section 302 (murder) and Section 309 IPC (abetment of suicide)
- The Court held that the right to die with dignity is part of the right to life under Article 21
- The Court established guidelines for passive euthanasia to be followed by High Courts on a case-by-case basis
- The petition to withdraw Aruna's feeding tube was rejected because KEM Hospital — as her caregiver — opposed it, and the Court found she was receiving adequate care
The judgment did not give Aruna the death her petition sought. But it gave India a legal framework it had never had before.
- 2009: Pinki Virani files the euthanasia petition before the Supreme Court
- 2010: Supreme Court appoints medical committee to evaluate Aruna's condition
- March 2011: Landmark SC judgment legalises passive euthanasia conditionally
- May 2015: Aruna Shanbaug dies of pneumonia at KEM Hospital
- March 2018: Supreme Court further strengthens the legal framework via Common Cause case
Passive vs Active Euthanasia: The Legal Distinction That Defines Everything
The distinction between passive and active euthanasia is not merely academic — it is the line that separates what is legal from what is criminal in India today.
Active euthanasia involves a direct, intentional act to end life — such as a doctor administering a lethal dose of medication. In India, this constitutes murder under Section 302 of the IPC (now Bharatiya Nyaya Sanhita) and remains categorically illegal. No court has the authority to permit it.
Passive euthanasia involves the withdrawal or withholding of life-sustaining treatment — removing a ventilator, stopping a feeding tube, or not initiating resuscitation — and allowing the disease or condition to take its natural course. The 2011 Aruna Shanbaug judgment established that this form is permissible under certain conditions.
The philosophical basis for this distinction lies in the acts vs. omissions doctrine: the law generally treats causing harm through action differently from allowing harm through inaction. Critics argue this distinction is morally arbitrary — if death is the intended outcome, the method should not determine legality. Supporters argue it preserves the sanctity of life while acknowledging limits to medical obligation.
Why this matters practically:
- Families of terminally ill patients can now legally seek withdrawal of ventilators/feeding tubes
- Hospitals cannot be prosecuted for stopping futile treatment under court-approved protocols
- Doctors are legally protected when they follow the established High Court procedure
- Patients in PVS without advance directives now have a legal pathway to passive euthanasia
Constitutional Foundations: Article 21 and the Right to Die
The constitutional heart of the euthanasia debate in India is Article 21: "No person shall be deprived of his life or personal liberty except according to procedure established by law."
The Supreme Court has, over decades, expansively interpreted Article 21 to include not just the right to live but the right to live with dignity. The question the Aruna Shanbaug case posed was: if Article 21 includes dignity in life, does it also include dignity in death?
The Court answered yes — but with conditions.
The 2018 Common Cause judgment by a five-judge constitutional bench finally settled what the 2011 judgment had left ambiguous: the right to die with dignity is a fundamental right under Article 21, enforceable through advance directives. This was a 9-judge bench reference and represents the highest constitutional authority on the subject.
- Article 21 is the constitutional anchor for all euthanasia jurisprudence in India
- Dignity in death has been elevated to a fundamental right
- The evolution from Gian Kaur (1996) to Common Cause (2018) represents a 22-year constitutional journey
- Article 14 (equality) and Article 19 (freedom) also inform the broader right-to-die framework
The 2018 Common Cause Judgment: India's Most Progressive Step on Euthanasia
If the 2011 Aruna Shanbaug judgment was the beginning, the 2018 Common Cause vs Union of India judgment (W.P. (Civil) No. 215 of 2005) was the culmination — at least for now.
A five-judge constitutional bench headed by Chief Justice Dipak Misra delivered a unanimous verdict that:
- Right to die with dignity is a fundamental right under Article 21
- Advance Directives (Living Wills) are legally valid in India
- A competent adult can execute a document specifying conditions under which they would not want life-sustaining treatment
- The Court revised and simplified the passive euthanasia procedure established in 2011
- Detailed guidelines were issued for the creation, storage, and enforcement of living wills
The judgment was groundbreaking because it shifted the framework from court-centric (where each case needed High Court approval) to individual-centric (where a person's pre-written instruction can guide medical decisions). According to the Supreme Court of India's official records, this judgment runs to over 500 pages across multiple opinions, making it one of the most comprehensive treatments of bioethics in Indian judicial history.
The 2018 verdict was welcomed by medical ethicists and patient rights advocates. However, implementation has remained patchy — awareness of living wills among the general public is still low, and healthcare systems in many states have not fully integrated the guidelines into practice.
Living Wills and Advance Directives: What They Are and How They Work in India
A living will (or advance directive) is a legal document in which a person, while mentally competent, specifies their wishes regarding medical treatment in the event they become incapacitated and unable to communicate.
In India, following the 2018 Common Cause judgment, the process for creating a valid advance directive includes:
How to Create a Valid Living Will in India
- The person must be an adult, mentally competent, and acting voluntarily
- The document must be signed by the person in the presence of two witnesses
- It must be countersigned by a Judicial Magistrate of First Class in the jurisdictional area
- A copy must be kept with the person's family and the local government hospital
When Does a Living Will Become Operative?
- The person must be terminally ill and unable to make decisions
- A Hospital Medical Board must confirm the condition
- A second opinion from a Board of Physicians nominated by the district collector is required
- The High Court must be informed (not required to approve, just informed)
- Only then can passive euthanasia — i.e., withdrawal of treatment — proceed
- A living will cannot authorise active euthanasia under any circumstances
- It applies only to withdrawal of life-sustaining treatment, not to causing death
- It can be revoked by the person at any time while competent
- The process is complex — legal reform advocacy is ongoing to simplify it
- Without a living will, the next of kin (with court oversight) makes the decision
Ethical and Philosophical Debates: The Core of the Euthanasia Controversy
The euthanasia debate is not just a legal question — it is a philosophical battleground where some of the deepest human values collide.
Arguments in Favour of Permitting Euthanasia
Autonomy: A person's right to make decisions about their own body is fundamental. Forcing a person to continue suffering against their will is a violation of individual dignity. Philosopher John Stuart Mill's harm principle holds that individuals should be free to act as they choose as long as they don't harm others — and choosing death harms no one but oneself, if at all.
Dignity: Death in a state of helplessness, pain, or persistent vegetative state is not dignified. Proponents argue that a dignified death — on one's own terms — is a form of mercy.
Medical Futility: When medical treatment can only prolong death rather than restore meaningful life, continuing it may be more about institutional inertia than patient welfare. Advance medical directives allow patients to define "meaningful life" for themselves.
Arguments Against Permitting Euthanasia
Sanctity of Life: Many religious traditions — Hinduism, Islam, Christianity — hold that human life is sacred and that only God or natural processes should determine its end. Deliberate ending of life, regardless of circumstances, violates this principle.
Slippery Slope: Critics warn that legalising euthanasia — even for terminal cases — creates pressure to expand it to cases of mental illness, disability, or elderly patients who feel like "burdens." Evidence from Belgium and the Netherlands shows how euthanasia criteria have expanded over time since legalisation.
Vulnerability and Coercion: Patients — especially the elderly, poor, or disabled — may feel pressured, explicitly or implicitly, to choose death to avoid burdening their families. The safeguards in law may be inadequate in practice.
Diagnostic Error: Medicine is not infallible. Patients declared in persistent vegetative states have, in rare documented cases, recovered consciousness. The National Institutes of Health and neurological research bodies have documented cases of "covert consciousness" in patients previously considered unresponsive.
The Medical Profession's Stance on Euthanasia in India
India's medical community is not monolithic on euthanasia — opinions range from strong support for passive euthanasia to categorical opposition to any form of assisted death.
The Indian Medical Association (IMA) has historically opposed active euthanasia on ethical grounds, citing the Hippocratic principle of primum non nocere (first, do no harm). However, the organisation has generally supported the concept of allowing natural death — through withdrawal of futile life support — in appropriate cases.
The 2018 Supreme Court judgment was broadly welcomed by palliative care specialists and intensivists, who regularly face end-of-life decisions in ICUs. Palliative care — focused on pain management and comfort for terminally ill patients — has grown significantly in India, but remains inadequate in rural areas.
Key challenges for the medical profession include:
- Fear of legal liability: Many doctors avoid withdrawing treatment even when medically warranted, fearing prosecution
- Family pressure: Indian families often insist on "doing everything possible," even when prognosis is hopeless
- Lack of awareness: Many clinicians are unfamiliar with the legal procedures established by the 2018 judgment
- Infrastructure gaps: Palliative care services are concentrated in urban centres, leaving rural patients with few options
The Supreme Court's guidelines attempted to protect doctors by creating a clear legal pathway — but implementation in hospitals across India remains uneven.
Euthanasia Laws: Global Perspectives
India's legal evolution on euthanasia places it in a specific position on the global spectrum — more progressive than many developing nations but still far behind countries that permit active euthanasia.
The Netherlands and Belgium represent the most permissive regimes. Both began with terminal physical illness criteria and have since expanded to include chronic psychiatric suffering — a trajectory that critics in India cite as a cautionary tale. Countries like the UK and most of Asia maintain prohibition on all forms of euthanasia, relying instead on palliative care to manage end-of-life suffering.
India's position — permitting passive but not active euthanasia — aligns with what several Commonwealth nations have adopted as a middle path.
Disadvantages, Risks, and Criticisms of Legalising Euthanasia
Even those who support compassionate end-of-life care often raise serious concerns about the risks of legalising euthanasia, particularly in a country like India.
1. Risk of Misuse and Elder Abuse: India has significant rates of elder neglect and familial financial disputes around inheritance. Legalised euthanasia — even passive — creates a potential vector for coerced or manipulated decisions that eliminate elderly relatives.
2. Weak Institutional Safeguards: India's legal and healthcare systems are under-resourced. The multi-step approval process established by the Supreme Court may work in metros but is practically inaccessible for patients in tier-2 cities, rural districts, or states with overburdened courts.
3. Diagnostic Uncertainty: As referenced earlier, PVS diagnosis is not always definitive. Premature withdrawal of treatment based on incorrect diagnosis could result in preventable deaths.
4. Conflict with Cultural Norms: Large sections of Indian society — across religious and caste communities — view prolonging life as a moral duty. Euthanasia decisions can fracture families and communities, particularly when some members consent and others oppose.
5. Inadequate Palliative Care Infrastructure: If the push for euthanasia is partly driven by the absence of good pain management and palliative care, the correct solution is to build that infrastructure — not to choose death as a default option for under-served patients.
6. Chilling Effect on Disabled Persons: Disability rights advocates globally have warned that legalised euthanasia sends a message that lives with severe disability are less worth living — normalising a hierarchy of human worth.
Government and Policy Response: India's Legal Framework Post-2018
Following the Common Cause judgment, the Ministry of Health and Family Welfare (MoHFW) was directed to develop guidelines consistent with the Supreme Court's ruling. The government initially resisted the advance directive framework, arguing it was difficult to implement at scale.
In 2023, the Supreme Court revised its 2018 guidelines to make the process for executing advance directives significantly simpler — removing the requirement for Judicial Magistrate countersignature and streamlining the medical board process. This was in response to petitions arguing that the original procedure was so cumbersome as to render living wills practically useless.
Key legal provisions governing euthanasia in India:
- Indian Penal Code / Bharatiya Nyaya Sanhita: Section 302 (murder) and Section 309 (attempt to suicide/abetment) govern the criminal dimensions
- Article 21, Constitution of India: Constitutional basis for the right to die with dignity
- Medical Council of India (now NMC) Regulations: Govern physician conduct in end-of-life decisions
- Aruna Shanbaug (2011) and Common Cause (2018) SC Judgments: Constitute the operative legal framework
India does not yet have a standalone euthanasia legislation — the law operates entirely through judicial precedent. Multiple law reform bodies, including the Law Commission of India, have recommended Parliament enact clear legislation, but no bill has been passed to date.
UPSC and Exam Relevance: What Aspirants Need to Know
The Aruna Shanbaug case and the broader euthanasia debate in India are highly relevant for:
- UPSC Mains — GS Paper 2: Judiciary, fundamental rights, health policy
- UPSC Mains — GS Paper 4: Ethics, medical ethics, compassion, rights of individuals
- UPSC Essay Paper: "Right to die is as fundamental as right to live" — a frequently discussed theme
- Law entrance exams and judicial services: Constitutional law, criminal law dimensions
- Medical ethics courses and PG medical exams
Previous Year Question relevance: UPSC 2015 Mains GS-2 asked about landmark SC judgments and right to life. UPSC Ethics paper has repeatedly tested candidates on end-of-life decisions, medical ethics, and the balance between compassion and law.
Future Outlook: Where Is India Headed on Euthanasia?
India's legal journey on euthanasia is unfinished. Several key developments are expected in the coming years:
1. Parliamentary Legislation: The absence of a statutory framework means the law rests entirely on judicial orders — which can be modified, misapplied, or inconsistently implemented. A dedicated End-of-Life Care Act would provide clarity, uniformity, and enforceable standards.
2. Expansion of Palliative Care: The National Health Policy 2017 recognised palliative care as a priority, but implementation has been slow. As palliative infrastructure improves, the pressure to consider euthanasia as an alternative to suffering may decrease — or the conversation may shift to what constitutes a dignified, pain-free natural death.
3. Technology and Consciousness Science: Advances in neuroimaging (such as functional MRI) are revealing that some patients in apparent PVS have covert awareness. This will likely prompt new legal and ethical questions about when a person is truly beyond recovery.
4. Active Euthanasia Debate: As neighbouring countries like Australia and Canada expand their frameworks, Indian courts and Parliament will face growing pressure from advocacy groups to revisit the absolute prohibition on active euthanasia. The debate is not closed — it is merely paused.
5. Awareness and Accessibility: Living wills remain unfamiliar to most Indians. Public awareness campaigns, simplified procedures, and hospital-based advance directive registries will be necessary for the 2018 judgment to have real-world impact.
How Students, Aspirants, and Professionals Can Use This Knowledge
For UPSC aspirants: Frame answers on euthanasia around the constitutional evolution — Gian Kaur (1996) → Aruna Shanbaug (2011) → Common Cause (2018). Connect it to GS-4 ethics questions about compassion, rights, and duties of the state.
For law students: Study the doctrinal shift in Article 21 interpretation. Analyse the act/omission distinction in criminal law and how the Court navigated it to permit passive euthanasia. Compare with UK Airedale NHS Trust vs Bland (1993) for a common law perspective.
For medical students and professionals: Understand the legal obligations under the 2018 advance directive guidelines. Know when a Hospital Medical Board referral is required and what the legal immunities are for doctors who follow proper procedure.
For researchers and policy analysts: Focus on the implementation gap — why are living wills still rare in India despite being legally valid since 2018? What reforms would make end-of-life legal frameworks accessible to ordinary citizens?
For general readers: The Aruna Shanbaug case is ultimately a story about human dignity, institutional failure (the perpetrator served only 7 years), and the extraordinary compassion of nurses who cared for a woman for 42 years. Whatever one's position on euthanasia, this case demands engagement with questions about what we owe each other as a society.
Frequently Asked Questions (FAQ)
1. Is euthanasia legal in India?
Passive euthanasia — the withdrawal of life-sustaining treatment from patients in irreversible conditions — is conditionally legal in India following the Supreme Court's 2011 judgment in the Aruna Shanbaug case and the 2018 Common Cause judgment. Active euthanasia, which involves a deliberate act to end life (such as a lethal injection), remains illegal and constitutes murder under Indian criminal law. India does not yet have a standalone euthanasia law; the framework is entirely court-created.
2. What was the Supreme Court's ruling in the Aruna Shanbaug case?
In March 2011, the Supreme Court ruled that passive euthanasia is permissible under certain conditions and established guidelines for High Courts to handle such petitions. The Court held that the right to die with dignity is part of the right to life guaranteed by Article 21. However, it rejected the specific petition to withdraw Aruna Shanbaug's feeding tube because her caregivers at KEM Hospital opposed it and she was receiving proper care.
3. What is a living will (advance directive) in India?
A living will is a legal document in which a mentally competent adult specifies their wishes about medical treatment — particularly life-sustaining treatment — in case they later become incapacitated. The Supreme Court validated living wills in the 2018 Common Cause judgment. In 2023, the Court simplified the procedure, removing the earlier requirement for a Judicial Magistrate's countersignature, making advance directives more accessible.
4. What is the difference between active and passive euthanasia?
Active euthanasia involves a direct act to end life — such as administering a lethal drug — and is illegal in India. Passive euthanasia involves withdrawing or withholding life-sustaining treatment (like a feeding tube or ventilator) and letting the condition take its natural course. The Supreme Court has held passive euthanasia permissible in specific circumstances. The distinction is foundational to Indian euthanasia law and mirrors the acts vs omissions principle in common law jurisprudence.
5. Why did Aruna Shanbaug's petition fail despite the Court legalising passive euthanasia?
The Court ruled that in non-voluntary euthanasia cases — where the patient cannot consent — the decision must be made by the "best friend" or nearest caregiver, not a third party. KEM Hospital, which had cared for Aruna for 36 years at the time of the petition, was considered her de facto family. Since the hospital staff opposed withdrawal of the feeding tube, the Court respected that choice and declined to order her death. The judgment legalised the framework but did not override the wishes of her actual caregivers.
6. Is the Aruna Shanbaug case relevant for UPSC?
Absolutely. The case intersects multiple UPSC syllabus areas: GS-2 (judiciary, fundamental rights, health policy), GS-4 (ethics, medical ethics, compassion, rights), and Essay topics on human dignity and right to die. Key facts — 2011 SC judgment, passive euthanasia, Article 21, and the 2018 Common Cause ruling — are frequently tested. Understanding the constitutional evolution from Gian Kaur (1996) to Common Cause (2018) is essential for a complete answer.
7. A common misconception: Does a living will mean a person can request active euthanasia?
No — this is a widespread misunderstanding. A living will in India can only specify that the person does not want life-sustaining treatment in certain terminal or irreversible conditions. It authorises passive euthanasia (letting nature take its course) — not active euthanasia (deliberate ending of life). No living will, court order, or family consent can make active euthanasia legal under current Indian law.
Conclusion: A Case That Will Echo Through Indian Law for Generations
The Aruna Shanbaug euthanasia case India is not merely a legal milestone — it is a mirror held up to Indian society, asking uncomfortable questions about justice, compassion, dignity, and what it means to be alive.
Five key takeaways define this debate: first, passive euthanasia is legal in India — active euthanasia is not; second, the right to die with dignity is now a constitutionally recognised fundamental right; third, living wills are valid and enforceable, though their reach remains limited in practice; fourth, the criminal justice system's failure in Aruna's original case — seven years for the perpetrator, 42 years for the victim — remains a wound that no legal verdict has healed; and fifth, this debate is far from over, as India must now decide whether it will legislate what courts have created, and whether it will ever cross the line from passive to active euthanasia.
Watch for developments in Parliamentary legislation and the growing palliative care movement — these will shape how India's end-of-life framework evolves in the next decade.
If this article helped you understand the Aruna Shanbaug case and India's euthanasia debate, bookmark it for revision, share it with fellow aspirants, and explore our related pieces on fundamental rights, landmark Supreme Court judgments, and medical ethics for your preparation.